
Secretory function of the small intestine. Parietal cell of the stomach: description, features and functions Digestion in the stomach
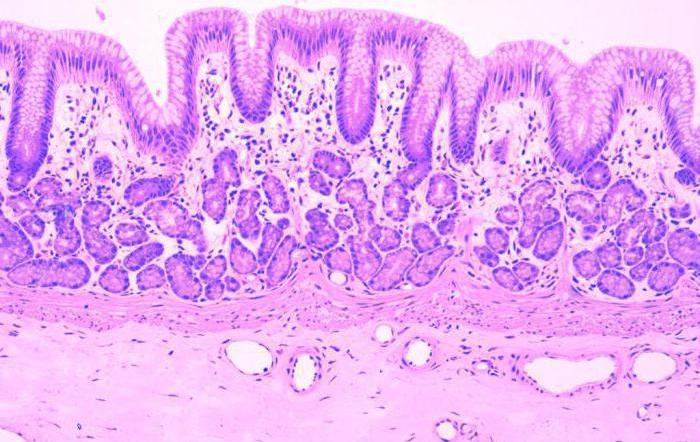
The pictures below show the gastric pit. A gastric pit (GD) is a groove or funnel-shaped invagination of the surface of the epithelium (E).
The surface epithelium consists of high prismatic mucous cells (MCs). lying on a common basement membrane (BM) with their own gastric glands (SG), which open and are visible in the depths of the dimple (see arrows). The basement membrane is often crossed by lymphocytes (L), penetrating from the lamina propria (LP) into the epithelium. In addition to lymphocytes, the lamina propria contains fibroblasts and fibrocytes (F), macrophages (Ma), plasma cells (PC) and a well-developed capillary network (Cap).
The superficial mucous cell, marked with an arrow, is shown in high magnification in Fig. 2.
To adjust the scale of the image of the cells in relation to the thickness of the entire gastric mucosa, the native glands are cut off below their necks. Cervical mucous cell (CMC). marked with an arrow, shown at high magnification in Fig. 3.
On sections of glands, one can distinguish parietal cells (PCs), protruding above the surface of the glands, and constantly rearranging chief cells (GCs). The capillary network (Cap) around one of the glands is also depicted.
PRISMATIC MUCOUS CELLS OF THE STOMACH
Rice. 2. Prismatic mucous cells (MCs) height from 20 to 40 nm, have an elliptical, basally located nucleus (N) with a prominent nucleolus, rich in heterochromatin. The cytoplasm contains rod-shaped mitochondria (M), a well-developed Golgi complex (G), centrioles, flattened cisterns of the granular endoplasmic reticulum, free lysosomes and a varying number of free ribosomes. In the apical part of the cell there are many osmiophilic PAS-positive, single-layer membrane-bound mucus droplets (MSD), which are synthesized in the Golgi complex. Vesicles containing glycosaminoglycans probably leave the cell body by diffusion; in the lumen of the gastric pit, mucigen vesicles are converted into acid-resistant mucus, which lubricates and protects the epithelium of the surface of the stomach from the digestive action gastric juice. The apical surface of the cell contains several short microvilli covered with glycocalyx (Gk). The basal pole of the cell lies on the basement membrane (BM).
Prismatic mucous cells connected to each other by well-developed junctional complexes (K), numerous lateral interdigitations and small desmosomes. Deeper in the dimple, the superficial mucous cells continue into the cervical mucous cells. The lifespan of mucous cells is about 3 days.
CERVICAL MUCOUS CELLS OF THE STOMACH
Rice. 3. Cervical mucous cells (CMCs) concentrated in the neck area of the stomach's own glands. These cells are pyramidal or pear-shaped and have an elliptical nucleus (N) with a prominent nucleolus. The cytoplasm contains rod-shaped mitochondria (M), a well-developed supranuclear Golgi complex (G), a small number of short cisternae of the granular endoplasmic reticulum, occasional lysosomes and a certain number of free ribosomes. The supranuclear part of the cell is occupied by large PAS-positive, moderately osmiophilic, secretory granules (SGs) surrounded by single-layer membranes, which contain glycosaminoglycans. The surface of the mucous cervical cells, facing the cavity of the dimple, bears short microvilli covered with glycocalyx (Gk). On the lateral surface there is a good lateral ridge-like interdigitations and junctional complexes are visible (K). The basal surface of the cell is adjacent to the basement membrane (BM).
Cervical mucous cells can also be found in the deep parts of the own gastric glands; they are also present in the cardiac and pyloric parts of the organ. The function of cervical mucous cells is still unknown. According to some scientists, they are undifferentiated replacement cells for superficial mucosal cells or progenitor cells for parietal and chief cells.
In Fig. Figure 1 to the left of the text shows the lower part of the body of the gastric gland (SG), cut transversely and longitudinally. In this case, a relatively constant zigzag direction of the gland cavity becomes visible. This is due to the mutual position of parietal cells (PCs) with chief cells (GCs). At the base of the gland the cavity is usually straight.
Three types of cells can be isolated in the body and base of the gastric gland. Starting from the top, these cells are marked with arrows and are shown on the right side in Fig. 2-4 at high magnification.
MAIN CELLS
Rice. 2. Chief cells (CH) are basophilic, from cubic to low prismatic in shape, localized in the lower third or lower half of the gland. The nucleus (N) is spherical, with a pronounced nucleolus, located in the basal part of the cell. The apical plasmalemma, covered with glycocalyx (Gk), forms short microvilli. Chief cells connect to neighboring cells using junctional complexes (K). The cytoplasm contains mitochondria, developed ergastoplasm (Ep) and a well-defined supranuclear Golgi complex (G).
Zymogen granules (ZGs) originate from the Golgi complex and then transform into mature secretory granules (SGs), accumulating at the apical pole of the cell. Then their contents, by fusion of the granule membranes with the apical plasmalemma, are released by exocytosis into the gland cavity. Chief cells produce pepsinogen, which is a precursor to the proteolytic enzyme pepsin.
PARIETAL CELLS
Rice. 3. Parietal cells (PC)- large pyramidal or spherical cells with bases protruding from outer surface body of the own gastric gland. Sometimes parietal cells contain many elliptical large mitochondria (M) with densely packed cristae, a Golgi complex, several short cisternae of the granular endoplasmic reticulum, a small number of tubules of the agranular endoplasmic reticulum, lysosomes and a few free ribosomes. Branched intracellular secretory tubules (ISCs) with a diameter of 1-2 nm begin as invaginations from the apical surface of the cell, surround the nucleus (N) and almost reach the basement membrane (BM) with its branches.
Many microvilli (MV) protrude into the tubules. Fine developed system plasmalemmal invaginations form a network of tubular-vascular profiles (T) with contents in the apical cytoplasm and around the tubules.
Severe acidophilia of parietal cells is the result of the accumulation of numerous mitochondria and smooth membranes. Parietal cells are connected by junctional complexes (J) and desmosomes to neighboring cells.
Parietal cells synthesize hydrochloric acid by a mechanism that is not fully understood. Most likely, tubular-vascular profiles actively transport chloride ions through the cell. Hydrogen ions released in the reaction of carbonic acid production and catalyzed by carbonic anhydride cross the plasmalemma by active transport, and then, together with chlorine ions, form 0.1 N. HCI.
Parietal cells produce intrinsic gastric factor, which is a glycoprotein responsible for the absorption of B12 in the small intestine. Erythroblasts cannot differentiate into mature forms without vitamin B12.
ENDOCRINE (ENTEROENDOCRINE, ENTEROCHROMAFFIN) CELLS
Rice. 4. Endocrine, enteroendocrine or enterochromaffin cells (EC) are localized at the base of the gastric glands. The cell body may have a triangular or polygonal nucleus (N), located at the apical pole of the cell. This cell pole rarely reaches the gland cavity. The cytoplasm contains small mitochondria, several short cisterns of the granular endoplasmic reticulum and the infranuclear Golgi complex, from which osmiophilic secretory granules (SG) with a diameter of 150-450 nm are separated. The granules are released by exocytosis from the cell body (arrow) to the capillaries. After crossing the basement membrane (BM), the granules become invisible. The granules produce argentaffin chromaffin reactions simultaneously, hence the term enterochromaffin cells. Endocrine cells are classified as APUD cells.

There are several classes of endocrine cells, with slight differences between them. NK cells produce the hormone serotonin, ECL cells produce histamine, G cells produce gastrin, which stimulates the production of HCl by parietal cells.
Stomach: histology, development and structure
The stomach is one of the main organs digestive tract. It processes all the products we consume. This is done thanks to hydrochloric acid, which is present in the stomach. This chemical compound is secreted by special cells. The structure of the stomach is represented by several types of tissues. In addition, the cells that secrete hydrochloric acid and other biologically active substances are not located throughout the organ. Therefore, anatomically, the stomach consists of several sections. Each of them differs in functional significance.
Stomach: organ histology
The stomach is a hollow, pouch-shaped organ. In addition to the chemical processing of chyme, it is necessary for the accumulation of food. To understand how digestion occurs, you should know what gastric histology is. This science studies the structure of organs at the tissue level. As you know, living matter consists of many cells. They, in turn, form tissues. The cells of the body are different in their structure. Therefore, the fabrics are also not the same. Each of them performs a specific function. Internal organs consist of several types of tissues. This ensures their activities.
The stomach is no exception. Histology studies the 4 layers of this organ. The first of these is the mucous membrane. It is located on the inner surface of the stomach. Next there is the submucosal layer. It is represented by adipose tissue, which contains blood and lymphatic vessels, as well as nerves. The next layer is the muscle layer. Thanks to it, the stomach can contract and relax. The last is the serous membrane. It is in contact with the abdominal cavity. Each of these layers is made up of cells that together form tissue.
Histology of the gastric mucosa
Normal histology of the gastric mucosa is represented by epithelial, glandular and lymphoid tissue. In addition, this shell contains a muscular plate consisting of smooth muscle. A feature of the mucous layer of the stomach is that there are many pits on its surface. They are located between the glands that secrete various biological substances. Next there is a layer of epithelial tissue. This is followed by the stomach gland. Together with lymphoid tissue, they form their own plate, which is part of the mucous membrane.
Glandular tissue has a certain structure. It is represented by several formations. Among them:
The secretory department consists of several exo- and endocrinocytes. The excretory duct of the glands of the mucous membrane exits into the bottom of the fossa located on the surface of the tissue. In addition, cells in this section are also capable of secreting mucus. The spaces between the glands are filled with coarse connective fibrous tissue.

Lymphoid elements may be present in the lamina propria of the mucous membrane. They are located diffusely, but throughout the surface. Next comes the muscle plate. It contains 2 layers of circular fibers and 1 layer of longitudinal fibers. He occupies an intermediate position.
Histological structure of the gastric epithelium
The upper layer of the mucous membrane, which is in contact with food masses, is the epithelium of the stomach. The histology of this section of the gastrointestinal tract differs from the structure of the tissue in the intestine. The epithelium not only protects the surface of the organ from damage, but also has a secretory function. This tissue lines the inside of the stomach cavity. It is located over the entire surface of the mucous membrane. Gastric pits are no exception.
The inner surface of the organ is covered with single-layer prismatic glandular epithelium. The cells of this tissue are secretory. They are called exocrinocytes. Together with the cells of the excretory ducts of the glands, they produce secretions.
Histology of the fundus of the stomach
The histology of different parts of the stomach is different. Anatomically, the organ is divided into several parts. Among them:
Big physiological significance has a fundic section of the stomach. The histology of this area is complex. The fundus contains the stomach's own glands. Their number is about 35 million. The depth of the pits between the fundic glands occupies 25% of the mucous membrane. The main function of this department is the production of hydrochloric acid. Under the influence of this substance, biological activation occurs active substances(pepsin), digestion of food, and also protects the body from bacterial and viral particles. Proprietary (fundic) glands consist of 2 types of cells - exo- and endocrinocytes.

Histology of the submucous membranes of the stomach
As in all organs, under the mucous membrane of the stomach there is a layer of fatty tissue. In its thickness there are vascular (venous and arterial) plexuses. They supply blood to the inner layers of the stomach wall. In particular, the muscular and submucosal membranes. In addition, this layer contains a network of lymphatic vessels and a nerve plexus. The muscular lining of the stomach is represented by three layers of muscle. This is a distinctive feature of this body. Longitudinal muscle fibers are located outside and inside. They have an oblique direction. Between them lies a layer of circular muscle fibers. As in the submucosa, there is a nerve plexus and a network of lymphatic vessels. The outside of the stomach is covered with a serous layer. It represents the visceral peritoneum.
Benign neoplasms of the stomach and intestines: histology of hemangioma
One of the benign neoplasms is hemangioma. Histology of the stomach and intestines is necessary for this disease. Indeed, despite the fact that the formation is benign, it should be differentiated from cancer. Histologically, hemangioma is represented by vascular tissue. The cells of this tumor are fully differentiated. They are no different from the elements that make up the arteries and veins of the body. Most often, gastric hemangioma forms in the submucosal layer. The typical location for this benign neoplasm is the pyloric region. The tumor can have different sizes.
In addition to the stomach, hemangiomas can be localized in the small and large intestines. These formations rarely make themselves felt. However, diagnosing hemangiomas is important. With large sizes and constant traumatization (chyme, feces) serious complications may occur. The main one is profuse gastrointestinal bleeding. It is difficult to suspect a benign neoplasm, since in most cases clinical manifestations are missing. An endoscopic examination reveals a dark red or bluish round spot rising above the mucous membrane. In this case, a diagnosis of hemangioma is made. The histology of the stomach and intestines is of decisive importance. In rare cases, hemangioma undergoes malignant transformation.
Gastric regeneration: histology in ulcer healing
One of the indications for histological examination is gastric ulcer. For this pathology, it is carried out endoscopic examination(FEGDS) with taking a biopsy. Histology is required if an ulcer is suspected of malignancy. Depending on the stage of the disease, the tissue obtained may vary. When the ulcer heals, the stomach scar is examined. In this case, histology is needed only if there are symptoms due to which malignant degeneration of the tissue can be suspected. If there is no malignancy, then the analysis reveals cells of coarse connective tissue. When a gastric ulcer becomes malignant, the histological picture may be different. It is characterized by changes in the cellular composition of the tissue and the presence of undifferentiated elements.
What is the purpose of gastric histology?
One of the organs of the digestive tract in which neoplasms often develop is the stomach. Histology should be performed if there is any change in the mucous membrane. The following diseases are considered indications for this study:

The listed pathologies refer to precancerous diseases. This does not mean that the patient has a malignant tumor and its location is the stomach. Histology helps determine exactly what changes are observed in the tissues of the organ. To prevent the development of malignant degeneration, it is worth conducting research as early as possible and taking action.
Gastric histology results
The results of histological examination may vary. If the organ tissue is not changed, then microscopy reveals normal prismatic single-layer glandular epithelium. When taking a biopsy of deeper layers, you can see smooth muscle fibers and adipocytes. If the patient has a scar from a protracted ulcer, then rough fibrous connective tissue is found. For benign formations, histological results may be different. They depend on the tissue from which the tumor developed (vascular, muscle, lymphoid). The main feature of benign formations is cell maturity.
Sampling of stomach tissue for histology: methodology
To perform a histological examination of stomach tissue, it is necessary to perform a biopsy of the organ. In most cases, it is performed using endoscopy. The apparatus for performing FEGDS is placed into the lumen of the stomach and several pieces of organ tissue are cut off. It is advisable to take biopsies from several distant sites. In some cases, tissue for histological examination is taken during surgery. After this, thin sections from the biopsy are taken in the laboratory and examined under a microscope.
How long does a histological analysis of stomach tissue take?
If you suspect oncological diseases gastric histology is required. How long does this analysis take? Only the attending physician can answer this question. On average, histology takes about 2 weeks. This applies to planned studies, for example, when removing a polyp.
During surgery, urgent histological examination of the tissue may be necessary. In this case, the analysis takes no more than half an hour.
Which clinics perform histological analysis?
Some patients are interested in: where can gastric histology be done urgently? This study is carried out in all clinics that have the necessary equipment and laboratory. Urgent histology is performed in oncology clinics, some surgical hospitals.
Atrophy of the gastric mucosa

Atrophy of the gastric mucosa - pathological process, developing as a result of inflammation. With atrophy, there is a gradual death of functioning cells and their replacement with scar tissue, and then its thinning.
Foci of atrophy can be detected in any gastritis, but in the classification of stomach diseases, a special form is distinguished - atrophic gastritis, for which such changes are most characteristic. It is important that this disease is a precancerous pathology. Therefore, all patients require treatment and medical supervision.
IN International Classification chronic atrophic gastritis is recorded under code K 29.4.
Characteristics of the atrophy process
The most common location for atrophy of the gastric mucosa is the lower third of the body or the antrum. One of the main damaging factors is considered to be Helicobacter, which lives closer to the pyloric zone.
At the initial stage, glandular (goblet) cells produce hydrochloric acid even in excess. Perhaps this process is associated with the stimulating effect of the bacterial enzyme system.
Then the synthesis of gastric juice is replaced by mucus, acidity gradually decreases.
By this time, the protective role of the mucous membrane is lost. Any food chemicals can harm the cells lining the inside of the stomach. Toxic products and remnants of destroyed cells become foreign to the body.
The autoimmune mechanism is involved in the destruction process. Antibodies are produced against damaged cells, which continue to fight their own epithelium. Important role plays a role in blocking recovery processes.
IN healthy stomach the epithelial layer is completely renewed every 6 days. Here, old dysfunctional cells remain in place or they are replaced with connective tissue.
On histology, instead of clear outlines of the epithelium (look along the upper edge), destroyed cells are visible, there are no pyriform glands
In any case, the atrophied mucosa cannot replace gastric juice with mucus. There is a gradual thinning of the stomach wall. In practice, the organ is excluded from digestion, and gastrin production increases. Food bolus enters the small intestine unprepared, which leads to failure of other successive stages.
The process doesn't end there. The most dangerous period atrophic changes: the epithelium begins to produce similar, but not true, cells. Most often they can be classified as intestinal. They are not able to produce gastric secretions. This process is called metaplasia and dysplasia (transformation), and precedes cancerous degeneration.
Atrophied areas on the mucosa cannot be completely restored, but with the help of treatment there is still a chance to support the remaining functioning cells, compensate for the lack of gastric juice and prevent disruption of the overall digestive process.
Reasons
Most common reasons diseases are considered: exposure to Helicobacter and autoimmune factors. Researchers have proposed distinguishing external (exogenous) and internal (endogenous) damage factors that can cause atrophic changes in the mucosa. External ones include toxic substances entering the stomach and malnutrition.
Toxic to the stomach are:
- nicotine, a decomposition product of tobacco products;
- dust particles of coal, cotton, metals;
- arsenic, lead salts;
- alcohol-containing liquids;
- medications from the Aspirin group, sulfonamides, corticosteroids.
- a person eats irregularly, periods of hunger alternate with overeating;
- mainly eat fast food, spicy and fatty dishes, “dry food”;
- cold or too hot food (ice cream, tea) enters the stomach;
- insufficiently chewed food in the mouth due to diseases of the teeth, gums, poor prosthetics, lack of teeth in old age.
- any disorders of the neuroendocrine regulation of secreting cells, leading to disruption of regeneration processes (stress, chronic diseases nervous system, myxedema, diabetes mellitus, dysfunction of the pituitary gland and adrenal glands);
- general human diseases that disrupt blood flow in the wall of the stomach and regional vessels (thrombosis, severe atherosclerosis), congestion in the veins against the background of increased pressure in the portal system;
- cardiac and respiratory failure accompanied by tissue hypoxia (lack of oxygen);
- deficiency of vitamin B 12 and iron in the body;
- hereditary predisposition - consists of a genetically determined lack of factors to restore the cellular composition of the mucosa.
- weight loss;
- symptoms of vitamin deficiency (dry skin, hair loss, bleeding gums, mouth ulcers, headaches);
- hormonal problems, expressed in men as impotence, in women as disrupted menstrual cycles, infertility;
- increased irritability, tearfulness, insomnia.
- focal atrophy - areas of atrophy with normal tissue alternate on the mucosa; this process is most favorable for treatment, because there are still cells capable of taking on a compensatory function;
- diffuse - a severe widespread process, covers the entire antrum and rises to the cardia, almost all cells are affected, instead of a mucous layer, continuous fibrosis appears.
Food can turn into exogenous damage factors if:
This "workaholic's dream" saturates the body, but is not a healthy food
TO internal reasons include:
Signs of atrophy
Symptoms of atrophy of the gastric mucosa appear late, when acidity reaches zero. Young and middle-aged men are more often affected. Pain syndrome is absent or very mild, which is why they consult a doctor at an advanced stage of the process.
Signs of atrophy do not differ from the general symptoms of gastric disorders. Patients note a feeling of heaviness in the epigastrium immediately after eating, sometimes nausea, belching, bloating, loud rumbling, bad breath and unstable stool.
Attacks of nausea and dyspeptic disorders are symptoms of pathology
The presence of signs of impaired digestion is indicated by:
Diagnostics
Atrophy of the gastric mucosa can only be diagnosed visually. It used to be determined by a pathologist or surgeon, but nowadays the widespread use of fibrogastroscopic technology makes it possible not only to record the picture in different parts of the stomach, but also to take material for histological examination, to divide the process into types and degrees of functional disorders.
Histologically, the infiltration of cells of the mucous layer by lymphocytes, destruction of the glandular epithelium, thinning of the wall, and impaired folding are revealed. Cracks and erosions may appear.
Depending on the size of the affected area, the following are distinguished:
Based on the number of lost and remaining healthy cells, the degrees of atrophic changes are distinguished:
With subatrophy, shortening of the cells of the epithelial layer is observed
Depending on the severity of the atrophic process, histological changes are assessed as:
In diagnosing pathology, it is not enough to establish that the gastric mucosa is atrophic; in order to try to stop the process, the doctor needs to know the cause of the changes, the degree of dysfunction of the organ.
For this, the patient undergoes next research: detection in the blood of antibodies to Helicobacter and to Castle factor (components of parietal cells), determination of the ratio of pepsinogen I, pepsinogen II (protein components for the production of hydrochloric acid), the method is considered a marker of atrophy, since it allows us to judge the remainder of intact epithelial glands.
It is also necessary to study gastrin 17, a hormonal substance responsible for the endocrine regulation of the secretion of epithelial cells, their restoration and motility. muscle tissue stomach and daily pH-metry to identify the nature of acid formation.
To identify Helicobacter, all patients with atrophic gastritis are prescribed a urease breath test by the attending physician.
What types of gastritis develop based on epithelial atrophy?
Depending on the degree of development and localization of the inflammation process in the stomach with mucosal atrophy, it is customary to distinguish several types of gastritis.
Surface
Most light form diseases. The acidity of gastric juice is almost normal. Happening copious discharge mucus glands, so protection is maintained. Histology shows signs of degeneration.
Focal
Acidity is maintained by areas of healthy epithelium. The mucous membrane shows alternating areas of atrophy and sclerosis with healthy tissue. Symptoms include intolerance to milk and eggs. This suggests a role for immune dysfunction.
Diffuse
The surface of the stomach is covered with a proliferation of immature cells, pits and ridges, and the structure of the mucosal glands is disrupted.
Erosive
In the atrophy zone, circulatory disturbance occurs, which gives a picture of spotty hemorrhages and accumulation of blood vessels. The course is severe with gastric bleeding. More often observed in alcoholics and people who have had a respiratory infection.
Antral
Named for the predominant localization of the lesion. It is characterized by cicatricial changes in the antral zone, narrowing of the pyloric region, and a tendency to develop into an ulcerative process.
Treatment
The problem of how to treat mucosal atrophy depends on the predominant aggressive action, the identified cause of the process, and the residual ability to recover (reparation). Given the absence of severe symptoms, patients are often treated on an outpatient basis. Mandatory recommendations include: regimen and diet.
It is not recommended to engage in strenuous sports; it is necessary to reduce physical activity to moderate. It is required to stop smoking and drinking alcoholic beverages, including beer. It is prohibited to take any medications without permission, including those for headaches and flu.
Diet Requirements
The patient's diet includes choosing foods that do not damage or irritate the gastric mucosa. Therefore, it is strictly prohibited:
The patient is advised to maintain meals in small, frequent meals. Use stewed, boiled, steamed, baked dishes. In case of pain, it is advised to switch to semi-liquid pureed food for several days (meatballs, low-fat broths, oatmeal on water, jelly).
If pain does not play a serious role in the clinic, then the diet should be varied, taking into account the given restrictions. Allowed:
The patient should consult a doctor regarding mineral water, since the choice depends on the acidity of the gastric juice, and it can vary during the process of atrophy.
Drug therapy
To restore the gastric mucosa, it is necessary to get rid of the harmful effects of Helicobacter, if present, and block a possible autoimmune process. To combat bacterial infection, a course of eradication is used.
A combination of tetracycline and penicillin series with Metronidazole (Trichopol). The course and dosage are chosen by the doctor individually.
Good results are accompanied by treatment with De-Nol (based on bismuth citrate)
To confirm the effectiveness, control studies are carried out on Helicobacter. In the initial stage of atrophy, when acidity may be increased, proton pump inhibitor drugs are recommended. They suppress the mechanism of hydrochloric acid production.
The group includes:
When hypo- and anacid states occur, these drugs are contraindicated. Acidin-pepsin and gastric juice are prescribed to replace one's own secretion. Stimulates the regeneration process Solcoseryl, Aloe in injections. Domperidone and prokinetics can support and improve gastric motor function.
Preparations based on bismuth and aluminum (Vicalin, Kaolin, bismuth nitrate) protect the mucous membrane from chemicals and bacteria from food products. If during the diagnostic process it becomes obvious that the body is in an autoimmune state, the patient is prescribed corticosteroid hormones to suppress an excessive immune response.
In severe cases of atrophy, the pathology is supplemented by a disruption in the production of enzymes by all organs involved in digestion. Therefore, enzymatic agents may be required: Panzinorm, Festal, Creon.
In case of B 12 deficiency anemia, courses of vitamin B 12 and folic acid are prescribed.
So far, the fibrogastroscopic method is the only most accessible way for patients to confirm the diagnosis of atrophy
Folk and herbal remedies
The traditional method of treatment should be approached with caution, taking into account acidity. With normal secretory function, you can take decoctions of chamomile and calendula.
If it is reduced, rosehip decoction and diluted juices of tomatoes, lemon, and potatoes are recommended to stimulate acid formation. At the pharmacy you can buy herbal teas with plantain, thyme, wormwood, and St. John's wort. It is convenient to use the herbal medicine Plantaglucid. It consists of granulated plantain extract, diluted in warm water before taking.
The most significant problem modern medicine is to identify patients and prevent cancer transformation. It is difficult to organize fibrogastroscopic examinations of patients if they have little concern. Members of a family in which a diagnosis has been detected are much more attentive to prevention. the only case atrophic gastritis and there are deaths from stomach cancer.
Such patients should undergo fibrogastroscopy once a year, follow a diet, stop smoking and drinking alcohol. No one can be sure what difficulties these people will have to overcome in life, and how their stomach will tolerate genetic predisposition.
The structure of the stomach wall
For readers of my blog who are interested in Human anatomy and physiology, we will present in detail structure of the stomach wall .
The stomach wall consists of the following layers:
I.Mucous membrane.
II. Submucosal layer.
III. Muscular membrane.
IV. Serous membrane.
I. Let's talk about the gastric mucosa.
The mucous membrane is represented by:
1. Single-layer, single-row, prismatic glandular (superficial pitted) epithelium.
2. Own muscle plate.
3. Basement membrane (lamina propria).
Note that the mucous membrane of the stomach is a continuation of the mucous membrane of the esophagus. At the junction of the esophagus and the stomach there is a serrated strip, which is the border between stratified epithelium mucous membrane of the esophagus and single-layer columnar epithelium stomach. The surface of the cells is covered with mucus synthesized by mucocytes.
Outwardly, it is noticeable that the mucous membrane is divided into small, 1-6 mm in diameter, protruding areas, which are called gastric fields. They have a polygonal shape and are separated from each other by grooves in which there are layers of connective tissue and superficial veins. In these fields there are special depressions - gastric dimples, 0.2 mm in diameter, surrounded by villous folds. These folds are most pronounced in the pyloric region. The openings of 1-2 ducts of the gastric glands open into each dimple.
Let's give some numbers. The thickness of the normal gastric mucosa is 0.25-1.5 mm. the total area is 500-800 cubic centimeters, and the number of glands can be from 4 to 25 million. On one square centimeter of the mucous membrane there are up to 60 gastric pits, and each pit contains 4-5 glands. The microvasculature of the gastric mucosa makes up 67-72% of the total gastric blood flow, the submucosal layer accounts for 13%, and the muscular layer accounts for 15%.
The mucous membrane forms folds that have different directions in different sections: along the lesser curvature there are longitudinal folds, in the area of the fundus and body of the stomach - transverse, oblique and longitudinal. They allow you to significantly increase the surface of the stomach, increase the area of contact of food with the mucous membrane and promote more efficient digestion.
Microscopically, three zones are distinguished in the gastric mucosa: cardiac, fundic and pyloric. The boundaries of these zones are unclear and they gradually transform into one another, with the width of the intermediate zones being about 1 cm. The zones basically coincide with the anatomical sections, but not completely. Each zone contains characteristic species glands:
- cardiac glands are located in the cardia region;
- the main glands of the stomach - in the area of the fundus and body of the stomach;
- intermediate gastric glands - in the mucous membrane of the intermediate part of the stomach, between the body and the pylorus;
- pyloric glands of the stomach - in the mucous membrane of the pylorus.
The superficial pitted epithelium of the mucosa is represented by cylindrical (prismatic) epithelial cells (mucocytes), arranged in one layer. The epithelial layer contains:
a) cells of the APUD system, in which biogenic amines and peptide hormones are synthesized, regulating the secretory and motor activity of the digestive organs, depending on the quantitative and qualitative composition of food;
b) intraepithelial lymphocytes: collect and transmit information about the antigenic properties of food to other cells of the immune system, have a cytotoxic effect against bacteria supplied with food.
The muscular plate of the mucous layer, together with the submucosal layer, creates the basis for the formation of numerous folds by the mucous membrane.
The basement membrane or lamina propria (stroma of the mucous membrane) is its own layer of loose connective tissue, in which blood and lymphatic vessels are located, forming the microvasculature, arteriole-venular shunts, fenestrated capillaries, gastric glands, intercellular substance represented by reticular, precollagen and collagen fibers and numerous cells:
— cells of lymphoid tissue - fibroblasts, reticular, mast, plasma cells, lymphocytes of varying degrees of maturity and granulocytes, united into reticular tissue or which can be represented by single and group follicles;
- granulocytes and lymphocytes migrating from the blood. They provide antibacterial and antitoxic effects and are involved in digestive leukopidesis. Let us dwell on digestive leukopidesis in more detail.
It is known that at the height of digestion in the lamina propria the number of basophils, neutrophils, eosinophils and lymphocytes increases significantly. In this case:
- basophils secrete compounds that increase vascular permeability and the number of intercellular substance. This causes swelling and loosening of the lamina propria, which promotes cell migration;
- neutrophils secrete hydrolytic enzymes (lysozyme, lactoferrin), which have an antibacterial effect;
— eosinophils and lymphocytes neutralize toxic substances due to their participation in local immune reactions.
Let's look at the functions of the eigenplate:
1. Support-mechanical.
Maintains the structure of the epithelial layer.
2. Transport-trophic.
Ensuring the diffusion of various compounds from the surface and epithelial cells into the blood.
3. Participates in digestive leukopidesis.
4. Lymphoid tissue of the lamina propria provides local protection against antigens of various natures (toxins, viruses, bacteria) that enter with food, carrying out phagocytosis and synthesis of immunoglobulins A.
II. The submucosal layer of the stomach wall is involved in the formation of folds and promotes stretching of the organ.
III. The muscular layer ensures gastric peristalsis, which allows for rhythmic movement of food. It is represented by three layers:
1. Longitudinal layer of muscles. It is a continuation of the longitudinal muscles of the esophagus and is located in the fundus and body of the stomach. More powerful bundles are located along the lesser curvature and especially increase in the area of the pylorus.
2. Circular layer. It is also a continuation of a similar layer of muscles of the esophagus, evenly covers the entire stomach, thins in the bottom area and thickens in the pyloric area, thereby forming the pyloric sphincter.
3. Inner oblique layer. Does not completely cover the stomach. Its main part first runs longitudinally, then forms an arc and goes to the greater curvature of the stomach. In the bottom area, the beams of this layer are mixed with the beams of the circular layer. One of the powerful muscle groups of this layer covers the cardia, and the other, the longest and most developed, is directed to the border between the body and the sinus and is called the lower segmental loop, which ensures the motor activity of the stomach during digestion.
IV. Serous membrane. or mesothelium, ensures the mobility of the stomach and reduces frictional resistance of the abdominal organs. It covers the entire anterior and posterior walls of the stomach, with the exception of a small area on the posterior wall at the cardia itself and along the greater and lesser curvature, as well as at the attachment points of the ligaments - there the peritoneum covering the stomach passes onto the ligaments and forms a duplicate.
The pictures below show the gastric pit. A gastric pit (GD) is a groove or funnel-shaped invagination of the surface of the epithelium (E).
The surface epithelium consists of high prismatic mucous cells (MCs), lying on a common basement membrane (BM) with their own gastric glands (SG), which open and are visible in the depths of the dimple (see arrows). The basement membrane is often crossed by lymphocytes (L), penetrating from the lamina propria (LP) into the epithelium. In addition to lymphocytes, the lamina propria contains fibroblasts and fibrocytes (F), macrophages (Ma), plasma cells (PC) and a well-developed capillary network (Cap).
The superficial mucous cell, marked with an arrow, is shown at high magnification in Fig. 2.
To adjust the scale of the image of the cells in relation to the thickness of the entire gastric mucosa, the native glands are cut off below their necks. Cervical mucous cell (CMC), marked with an arrow, is shown at high magnification in Fig. 3.
On sections of glands, one can distinguish parietal cells (PCs), protruding above the surface of the glands, and constantly rearranging chief cells (GCs). The capillary network (Cap) around one of the glands is also depicted. 
Rice. 2. Prismatic mucous cells (MCs) height from 20 to 40 nm, have an elliptical, basally located nucleus (N) with a prominent nucleolus, rich in heterochromatin. The cytoplasm contains rod-shaped mitochondria (M), a well-developed Golgi complex (G), centrioles, flattened cisterns of the granular endoplasmic reticulum, free lysosomes and a varying number of free ribosomes. In the apical part of the cell there are many osmiophilic PAS-positive, single-layer membrane-bound mucus droplets (MSD), which are synthesized in the Golgi complex. Vesicles containing glycosaminoglycans probably leave the cell body by diffusion; in the lumen of the gastric pit, mucigen vesicles are converted into acid-resistant mucus, which lubricates and protects the epithelium of the surface of the stomach from the digestive action of gastric juice. The apical surface of the cell contains several short microvilli covered with glycocalyx (Gk). The basal pole of the cell lies on the basement membrane (BM).
Prismatic mucous cells connected to each other by well-developed junctional complexes (K), numerous lateral interdigitations and small desmosomes. Deeper in the dimple, the superficial mucous cells continue into the cervical mucous cells. The lifespan of mucous cells is about 3 days.
Rice. 3. Cervical mucous cells (CMCs) concentrated in the neck area of the stomach's own glands. These cells are pyramidal or pear-shaped and have an elliptical nucleus (N) with a prominent nucleolus. The cytoplasm contains rod-shaped mitochondria (M), a well-developed supranuclear Golgi complex (G), a small number of short cisternae of the granular endoplasmic reticulum, occasional lysosomes and a certain number of free ribosomes. The supranuclear part of the cell is occupied by large PAS-positive, moderately osmiophilic, secretory granules (SGs) surrounded by single-layer membranes, which contain glycosaminoglycans. The surface of the mucous cervical cells, facing the cavity of the dimple, bears short microvilli covered with glycocalyx (Gk). On the lateral surface there is a good lateral ridge-like interdigitations and junctional complexes are visible (K). The basal surface of the cell is adjacent to the basement membrane (BM).
Cervical mucous cells can also be found in the deep parts of the own gastric glands; they are also present in the cardiac and pyloric parts of the organ. The function of cervical mucous cells is still unknown. According to some scientists, they are undifferentiated replacement cells for superficial mucosal cells or progenitor cells for parietal and chief cells.
In Fig. Figure 1 to the left of the text shows the lower part of the body of the gastric gland (SG), cut transversely and longitudinally. In this case, a relatively constant zigzag direction of the gland cavity becomes visible. This is due to the mutual position of parietal cells (PCs) with chief cells (GCs). At the base of the gland the cavity is usually straight.

The glandular epithelium is located on the basement membrane, which is removed in the cross section. A dense capillary network (Cap), closely surrounding the gland, is located lateral to the basement membrane. Pericytes (P) covering the capillaries are easily visible.
Three types of cells can be isolated in the body and base of the gastric gland. Starting from the top, these cells are marked with arrows and are shown on the right side in Fig. 2-4 at high magnification.
Rice. 2. Chief cells (CH) are basophilic, from cubic to low prismatic in shape, localized in the lower third or lower half of the gland. The nucleus (N) is spherical, with a pronounced nucleolus, located in the basal part of the cell. The apical plasmalemma, covered with glycocalyx (Gk), forms short microvilli. Chief cells connect to neighboring cells using junctional complexes (K). The cytoplasm contains mitochondria, developed ergastoplasm (Ep) and a well-defined supranuclear Golgi complex (G).
Zymogen granules (ZGs) originate from the Golgi complex and then transform into mature secretory granules (SGs), accumulating at the apical pole of the cell. Then their contents, by fusion of the granule membranes with the apical plasmalemma, are released by exocytosis into the gland cavity. Chief cells produce pepsinogen, which is a precursor to the proteolytic enzyme pepsin.
Rice. 3. Parietal cells (PC)- large pyramidal or spherical cells with bases protruding from the outer surface of the body of the gastric gland. Sometimes parietal cells contain many elliptical large mitochondria (M) with densely packed cristae, a Golgi complex, several short cisternae of the granular endoplasmic reticulum, a small number of tubules of the agranular endoplasmic reticulum, lysosomes and a few free ribosomes. Branched intracellular secretory tubules (ISCs) with a diameter of 1-2 nm begin as invaginations from the apical surface of the cell, surround the nucleus (N) and almost reach the basement membrane (BM) with its branches.
Many microvilli (MV) protrude into the tubules. A well-developed system of plasmalemmal invaginations forms a network of tubular-vascular profiles (T) with contents in the apical cytoplasm and around the tubules.
Severe acidophilia of parietal cells is the result of the accumulation of numerous mitochondria and smooth membranes. Parietal cells are connected by junctional complexes (J) and desmosomes to neighboring cells.
Parietal cells synthesize hydrochloric acid by a mechanism that is not fully understood. Most likely, tubular-vascular profiles actively transport chloride ions through the cell. Hydrogen ions released in the reaction of carbonic acid production and catalyzed by carbonic anhydride cross the plasmalemma by active transport, and then, together with chlorine ions, form 0.1 N. HCI.
Parietal cells produce intrinsic gastric factor, which is a glycoprotein responsible for the absorption of B12 in the small intestine. Erythroblasts cannot differentiate into mature forms without vitamin B12.
Rice. 4. Endocrine, enteroendocrine or enterochromaffin cells (EC) are localized at the base of the gastric glands. The cell body may have a triangular or polygonal nucleus (N), located at the apical pole of the cell. This cell pole rarely reaches the gland cavity. The cytoplasm contains small mitochondria, several short cisterns of the granular endoplasmic reticulum and the infranuclear Golgi complex, from which osmiophilic secretory granules (SG) with a diameter of 150-450 nm are separated. The granules are released by exocytosis from the cell body (arrow) to the capillaries. After crossing the basement membrane (BM), the granules become invisible. The granules produce argentaffin chromaffin reactions simultaneously, hence the term enterochromaffin cells. Endocrine cells are classified as APUD cells.
There are several classes of endocrine cells, with slight differences between them. NK cells produce the hormone serotonin, ECL cells produce histamine, G cells produce gastrin, which stimulates the production of HCl by parietal cells.

INTESTINES
The intestine consists of two parts - the large and small intestines. It continues the process of food digestion, which began in the overlying sections of the digestive tube.
The small intestine reaches 4-5 m in length, consists of three sections: duodenum (30 cm), jejunum (2 m) and ileum (3 m) and performs the following functions:
1. Digestive: under the influence of its own enzymes and pancreatic enzymes, proteins (enterokinase, trypsin, erypsin), lipids (lipase), carbohydrates (amylase, maltase, sucrase, lactase) and nucleoproteins (nuclease) are broken down.
2. Secretory: secretion of intestinal juice: consists of water, enzymes (dipeptidases), minerals, mucus.
3. absorption of nutrient breakdown products. To increase the absorption surface, the intestinal mucosa has villi, and epithelial cells have a brush border.
4. Motor-evacuation function, which consists in mixing the chyme and moving it into the underlying sections of the intestine.
5. Barrier-protective. The basis of the latter is secreted mucus, integumentary epithelium, lymphoid follicles and immunocompetent cells.
6. Endocrine: production by endocrinocytes of the APUD system of various hormones that provide regulation of the secretion of intestinal juice, blood supply, motility, etc.
Structure. Wall small intestine formed by three membranes: mucous, muscular and serous. The mucous membrane consists of epithelium, lamina propria, muscularis lamina and submucosa. A feature of the relief of the mucous membrane of the small intestine is the presence of circular folds, villi and crypts, which increase the total surface of the small intestine, which facilitates the performance of its main functions.
Circular folds are protrusions of the mucous membrane into the intestinal cavity.
Intestinal villi are finger-shaped protrusions into the lumen of the intestine of the lamina propria of the mucosa, covered with epithelium. In the loose fibrous connective tissue located under the basement membrane of the epithelium there is a dense network of blood capillaries, and in the center of the villus there is a lymphatic capillary. In the stroma of the villi there are also single smooth myocytes that ensure the movement of the villi and contribute to the process of moving food breakdown products absorbed into the blood and lymph. The surface of the villi is covered with single-layer columnar bordered epithelium. It consists of three types of cells; bordered epithelial cells, goblet cells and endocrine cells.
Bordered epithelial cells are the most numerous and have a pronounced polarity of structure. The apical surface contains microvilli, about 1 µm in height and 0.1 µm in diameter. Their number in a cell reaches 2-3 thousand and together they form a border that increases the absorption surface of the mucosa by 30-40 times. On the surface of the microvilli there is a glycocalyx, represented by lipoproteins and glycoproteins. The membrane and glycocalyx of microvilli contain a large number of enzymes involved in parietal and membrane digestion, as well as taking part in the absorption function of the resulting monomers (glucose, amino acids). Fats are absorbed by phagocytosis or in the form of their constituent components - glycerol and fatty acids. The cytoplasm contains developed cytoplasmic reticulum, Golgi complex, mitochondria, and lysosomal apparatus. Membranes in the apical part of adjacent epithelial cells form end plates that prevent the penetration of substances from the intestinal cavity.
Goblet cells in the villi are located singly between the bordered epithelial cells and produce a mucous secretion. They have the shape of a glass, in the expanded apical part of which secretory granules with mucous contents are located. The latter, released on the surface of the mucous membrane, moisturize it, which promotes the movement of chyme along the intestines.
Endocrinocytes, like goblet cells, are scattered singly between the bordered epithelial cells.
Crypts are tubular ingrowths of the epithelium into the lamina propria of the mucosa. Their lumen opens between the bases of neighboring villi. In the small intestine, their number is about 150 million. Among the epithelial cells of the crypts, in addition to those mentioned above, the epithelium of the villi (bordered, goblet, endocrine) contains cells without a border and cells with acidophilic granulation (Paneth cells). All of these cells, in contrast to those of the villi, have a smaller height, a thinner striated border and a more basophilic cytoplasm. Cells lacking a border are a population of poorly differentiated cells that are the source of physiological regeneration of the crypt and villi epithelium. As these cells proliferate and differentiate, they move from the base of the crypts to the tip of the villi, replacing cells that have completed the cell cycle. Complete replacement of villous epithelial cells thus takes place in 3-5 days.
Paneth cells are located in groups at the base of the crypts. These are prismatic cells, in the apical part of which there are large acidophilic (ranulae). The cell nuclei and cytoplasmic reticulum are shifted to the basal pole. The secretory product of these cells are dipeptidases - enzymes that break down dipeptides into amino acids. It is believed that these cells also produce lysozyme, which destroys cell membranes bacteria.
Endocrinocytes. EC cells are divided into EC 1 and EC 2 cells. The former produce the hormone melatonin and serotonin, the latter produce motilin and substance P. Motilin stimulates the motor activity of the villi. Substance P regulates the blood supply to the mucous membrane. Serotonin stimulates mucus production and affects blood supply and intestinal motility. Melatonin is responsible for biorhythms of functioning depending on the time of day (lighting).
ECL cells produce histamine, which stimulates the chief and parietal cells of the stomach.
A-cells produce enteroglucagon, which increases blood sugar levels and stimulates mucus production by the integumentary epithelium of the stomach.
G cells produce gastrin, which stimulates the chief and parietal cells of the stomach.
D cells produce somatostatin, and D 1 cells produce vasointestinal polypeptide (VIP). Somatostatin suppresses gland secretion and cell division, VIP - relaxes smooth muscles, dilates blood vessels, lowers blood pressure.
S cells produce secretin, which stimulates the secretion of bicarbonate by the pancreas.
I-cells produce pancreozymin, which stimulates the pancreas, and cholecystokinin, which causes contraction of the gallbladder.
The lamina propria of the mucous membrane of the small intestine is formed by loose, unformed connective tissue with the presence of a large number of reticular and elastic fibers, plexuses of hemo- and lymphocapillaries. Lymphatic follicles are also found. The number of the latter towards the ileum increases. There are more of them in children than in adults. In addition to lymphocytes, plasma cells and eosinophils are found in the lamina propria. The muscular plate of the mucous membrane is poorly developed and is represented by internal circular and external longitudinal muscle layers.
The submucosa is formed by loose, unformed connective tissue, in which there is a plexus of blood and lymphatic vessels and nerve plexuses(submucosal). The end sections of the duodenal (Bruner's) glands are located in the duodenum. In structure, these are complex branched tubular glands. The terminal sections are formed by mucocytes and a few apical granular cells (Packet cells).
The muscularis propria consists of two layers of smooth muscle tissue: the inner circular and the outer longitudinal. Both layers have a spiral orientation. Between the layers in the layer of connective tissue lie the intermuscular vascular and nerve plexuses, which provide peristaltic movement.
The serosa is formed by an underlying connective tissue base covered with mesothelium.
Histophysiology of digestion and absorption processes in small intestine
There are cavity, parietal, membrane and intracellular digestion. Cavity digestion is carried out with the help of enzymes of the digestive glands (salivary, gastric, pancreatic and intestinal). Parietal digestion breaks down food in the mucus layer covering the villi. Membrane digestion occurs in the glycocalyx of the brush border of villous enterocytes. Intracellular - inside enterocytes, through phagocytosis and pinocytosis.
The main structure that facilitates digestion and absorption in the small intestine is the villi. The latter, due to the presence of smooth myocytes in the stroma, contract and function as a pump.
Carbohydrates are absorbed after being broken down into monosaccharides (glucose), which is absorbed through the microvilli membrane with the help of a carrier protein. Proteins are absorbed in a similar way, after they are broken down into amino acids. Fats in the intestinal cavity, under the influence of bile acids, undergo emulsification (to fat droplets no more than 0.5 microns). Small droplets of fat are adsorbed by the glycocalyx of enterocytes, and then, under the influence of lipases, the fat is broken down into glycerol and fatty acids. Fatty acids combine with cholesterol (esterification), after which they easily penetrate into the cell. In the agranular cytoplasmic reticulum of enterocytes, fatty acids are recombined with absorbed glycerol to form body-specific fats. Protein and carbohydrate components are sequentially attached to the latter in the granular cytoplasmic reticulum and the Golgi complex. The resulting complex compounds in the Golgi complex are formed into granules surrounded by a membrane (chylomicrons). They contain more than 80% triglycerides, cholesterol (8%), phospholipids (7%), protein (2%), etc. By exocytosis, they are secreted by the epithelium through the lateral surface of epithelial cells into the intercellular spaces, from where they enter the lymphocapillaries of the villi.
The structural features of the sections of the small intestine in the caudal direction of the villi become longer and thinner, and the number of goblet cells in the epithelium increases. In the lamina propria the number of lymphoid follicles increases, they form clusters - Peyer's patches Duodenal glands in the jejunum and ileum are missing.
The human stomach contains glands that digest food. These include parietal cells. At normal operation glands, a person does not experience any unpleasant or painful sensations. For the body to function properly it requires proper nutrition. If a person often eats junk food, then the gastric glands, including parietal cells, suffer.
Digestion in the stomach
The stomach consists of three parts:
- cardiac - located near the esophagus;
- fundamental - the main part;
- pyloric - near the duodenum.
Inside there is a mucous membrane that is the first to come into contact with food coming from the esophagus. In addition, there is a muscular and serous membrane. They are responsible for motor and protective functions.
The mucous membrane contains an epithelial layer, which contains a large number of glands. They secrete a secretion that allows them to digest food. Gastric juice is produced constantly, but its amount is influenced by hormones and the brain. Thoughts about food and the smell make the glands work more actively. Thanks to this, up to 3 liters of secretion are produced per day.
Types of stomach glands
The glands in the stomach have a variety of shapes. The number is in the millions. Each gland has its own function. They come in the following types:

What is a parietal cell
The cell is shaped like a cone or pyramid. The number is higher in men than in women. Parietal cells secrete hydrochloric acid. For the process to occur, the participation of histamine, gastrin and acetylcholine is required. They act on the cell through special receptors. The amount of hydrochloric acid is regulated by the nervous system.
Previously, in case of gastric ulcer, part of the organ was removed for better functioning. But in practice it turned out that if the part in which the parietal cells were located was cut out, then digestion slowed down. The patient had complications after surgery. At the moment, this method of treatment has been abandoned.
Features and Functions
Distinctive feature parietal cells are their single location outside the mucous cells. They are larger than other epithelial cells. Their appearance is asymmetrical; the cytoplasm contains one or two nuclei.
Inside the cells there are tubules responsible for transporting ions. From the inside, the channels go into external environment cells and open the lumen of the gland. There are villi on the surface, microvilli are located inside the tubules. Another feature of cells is a large number of mitochondria. The main function of parietal cells is to produce ions that contain hydrochloric acid.
Hydrochloric acid is required to destroy pathogenic bacteria and reduce the rotting of food debris. Thanks to it, the digestion process goes faster, proteins are absorbed more easily.

Factors affecting the functioning of the glands
The following factors influence the proper functioning of the gastric glands:
- healthy eating;
- emotional state of a person;
- stressful situations;
- chronic diseases of the liver and gall bladder;
- alcohol abuse;
- long-term use drugs that irritate receptors;
- chronic gastritis;
- stomach ulcer;
- smoking.
When work is disrupted, chronic diseases occur. Failure to follow the rules of a healthy lifestyle provokes the risk of healthy cells degenerating into malignant neoplasms. Stomach cancer is not immediately recognized. The fact is that the process begins gradually, and the patient does not see a doctor for a long time.
The work of the glands is important for the digestion of food, so it is important to prevent the development of stomach diseases and undergo regular medical examinations and avoid surgery whenever possible.

Autoimmune gastritis
Sometimes a person develops a Disease in which the body perceives its own cells as enemies and begins to destroy them. In practice, such gastritis is rare and is characterized by the death of the gastric mucosa and the destruction of the gastric glands.
As a result of a malfunction in the body, the production of gastric juice is reduced, and problems arise with the digestion of food. At the same time, the level of internal Castle factor decreases and vitamin B12 deficiency appears, which leads to the development of anemia.
Typically, autoimmune gastritis develops into a chronic form. In this case, the patient experiences concomitant diseases thyroid gland. The disease is difficult to diagnose and cannot be completely cured. Patients take medications throughout their lives.
The appearance of antibodies to Castle factor and parietal cells is detected by immunoglobulins, which indicate that vitamin B12 has ceased to be absorbed.

Causes and symptoms of autoimmune gastritis
The exact causes of the development of this disease are still unknown. But there are a number of assumptions explaining what can trigger the process of self-destruction in the body:

The symptoms of the disease differ little from other diseases of the gastrointestinal tract. First of all, patients pay attention to:
- pain in the stomach;
- heaviness and discomfort after eating;
- nausea;
- bowel dysfunction;
- belching;
- rumbling in the stomach;
- constant flatulence.
In addition to the main signs, a person may be tormented by symptoms to which he does not attach importance. Low blood pressure, constant fatigue, sweating, weight loss and pale skin are secondary signs of the disease. From doctors main reason, indicating autoimmune gastritis, is the condition that antibodies to parietal cells are elevated.
Diagnosis and treatment of autoimmune gastritis
To make a diagnosis, the doctor collects data about the patient. Anamnesis and current complaints suggest what disease is tormenting the person. To confirm or refute the diagnosis, the following measures are required:
- general and biochemical analysis blood;
- immunological analysis for antibodies to parietal cells;
- level of gastric juice secretion;
- FGDS;
- Ultrasound internal organs;
- determination of vitamin B12 levels.
Based on the examination, the doctor determines the diagnosis. Autoimmune gastritis cannot be treated. All drugs are aimed at reducing discomfort and improving quality of life.
For severe pain, painkillers and antispasmodics are prescribed. Additionally, it is necessary to take enzymes to improve food digestion. A course of B vitamins and folic acid is taken. A diet is prescribed that excludes foods that have a negative effect on the gastric mucosa.
The normal residence time of the contents (digested food) in the stomach is about 1 hour.
Anatomy of the stomach
Anatomically, the stomach is divided into four parts:- cardiac(lat. pars cardiaca), adjacent to the esophagus;
- pyloric or gatekeeper (lat. pars pylorica), adjacent to the duodenum;
- body of stomach(lat. corpus ventriculi), located between the cardiac and pyloric parts;
- fundus of the stomach(lat. fundus ventriculi), located above and to the left of the cardiac part.
The figure on the right shows: 1. Body of the stomach. 2. Fundus of the stomach. 3. Anterior wall of the stomach. 4. Greater curvature. 5. Small curvature. 6. Lower esophageal sphincter (cardia). 9. Pyloric sphincter. 10. Antrum. 11. Pyloric canal. 12. Corner cut. 13. A groove formed during digestion between the longitudinal folds of the mucosa along the lesser curvature. 14. Folds of the mucous membrane.
The following anatomical structures are also distinguished in the stomach:
- anterior wall of the stomach(lat. paries anterior);
- posterior wall of the stomach(lat. paries posterior);
- lesser curvature of the stomach(lat. curvatura ventriculi minor);
- greater curvature of the stomach(lat. curvatura ventriculi major).
The shape of the stomach depends on the position of the body, the fullness of food, and the functional state of the person. With average filling, the length of the stomach is 14–30 cm, width 10–16 cm, length of the lesser curvature 10.5 cm, greater curvature 32–64 cm, wall thickness in the cardiac region 2–3 mm (up to 6 mm), in antrum 3–4 mm (up to 8 mm). The stomach capacity is from 1.5 to 2.5 liters (the male stomach is larger than the female). The normal weight of the stomach of a “conditional person” (with a body weight of 70 kg) is 150 g.

The stomach wall consists of four main layers (listed from the inner surface of the wall to the outer):
- mucous membrane covered with single-layer columnar epithelium
- submucosa
- muscle layer, consisting of three sublayers of smooth muscle:
- inner sublayer of oblique muscles
- middle sublayer of circular muscles
- outer sublayer of longitudinal muscles
- serous membrane.
Stomach mucosa
 The mucous membrane of the stomach is formed by a single-layer columnar epithelium, a layer of its own and a muscular plate that forms folds (relief of the mucous membrane), gastric fields and gastric pits, where the excretory ducts of the gastric glands are localized. In the proper layer of the mucous membrane there are tubular gastric glands, consisting of parietal cells that produce hydrochloric acid; main cells producing the proenzyme pepsin pepsinogen, and accessory (mucosal) cells secreting mucus. In addition, mucus is synthesized by mucous cells located in the layer of the surface (integumentary) epithelium of the stomach.
The mucous membrane of the stomach is formed by a single-layer columnar epithelium, a layer of its own and a muscular plate that forms folds (relief of the mucous membrane), gastric fields and gastric pits, where the excretory ducts of the gastric glands are localized. In the proper layer of the mucous membrane there are tubular gastric glands, consisting of parietal cells that produce hydrochloric acid; main cells producing the proenzyme pepsin pepsinogen, and accessory (mucosal) cells secreting mucus. In addition, mucus is synthesized by mucous cells located in the layer of the surface (integumentary) epithelium of the stomach. The surface of the gastric mucosa is covered with a continuous thin layer of mucous gel consisting of glycoproteins, and underneath is a layer of bicarbonates adjacent to the superficial epithelium of the mucosa. Together they form the mucobicarbonate barrier of the stomach, which protects epithelial cells from the aggression of the acid-peptic factor (Y.S. Zimmerman). The mucus contains antimicrobial activity immunoglobulin A (IgA), lysozyme, lactoferrin and other components.
The surface of the mucous membrane of the body of the stomach has a pitted structure, which creates conditions for minimal contact of the epithelium with the aggressive intracavitary environment of the stomach, which is also facilitated by a thick layer of mucous gel. Therefore, the acidity on the surface of the epithelium is close to neutral.  The mucous membrane of the body of the stomach is characterized by a relatively short path for the movement of hydrochloric acid from the parietal cells into the lumen of the stomach, since they are located mainly in the upper half of the glands, and the main cells are in the basal part. An important contribution to the mechanism of protecting the gastric mucosa from the aggression of gastric juice is made by the extremely rapid nature of gland secretion, caused by the work of the muscle fibers of the gastric mucosa. On the contrary, the mucous membrane of the antral region of the stomach (see the figure on the right) is characterized by a “villous” structure of the surface of the mucous membrane, which is formed by short villi or convoluted ridges 125–350 µm high (Lysikov Yu.A. et al.).
The mucous membrane of the body of the stomach is characterized by a relatively short path for the movement of hydrochloric acid from the parietal cells into the lumen of the stomach, since they are located mainly in the upper half of the glands, and the main cells are in the basal part. An important contribution to the mechanism of protecting the gastric mucosa from the aggression of gastric juice is made by the extremely rapid nature of gland secretion, caused by the work of the muscle fibers of the gastric mucosa. On the contrary, the mucous membrane of the antral region of the stomach (see the figure on the right) is characterized by a “villous” structure of the surface of the mucous membrane, which is formed by short villi or convoluted ridges 125–350 µm high (Lysikov Yu.A. et al.).
Stomach in children
In children, the shape of the stomach is not constant and depends on the constitution of the child’s body, age and diet. In newborns, the stomach has a round shape; by the beginning of the first year it becomes oblong. By the age of 7–11, a child’s stomach does not differ in shape from an adult’s. In children infancy the stomach is positioned horizontally, but as soon as the child begins to walk, it takes on a more vertical position.By the birth of a child, the fundus and cardiac part of the stomach are not sufficiently developed, and the pyloric part is much better, which explains frequent regurgitation. Regurgitation is also promoted by swallowing air during sucking (aerophagia), with improper feeding technique, short frenulum of the tongue, greedy sucking, and too rapid release of milk from the mother's breast.
Gastric juice
The main components of gastric juice are: hydrochloric acid secreted by parietal cells, proteolytic enzymes produced by chief cells and non-proteolytic enzymes, mucus and bicarbonates (secreted by accessory cells), intrinsic Castle factor (production of parietal cells).The gastric juice of a healthy person is practically colorless, odorless and contains a small amount of mucus.
Basal secretion, not stimulated by food or otherwise, in men is: gastric juice 80-100 ml/h, hydrochloric acid - 2.5-5.0 mmol/h, pepsin - 20-35 mg/h. Women have 25–30% less. About 2 liters of gastric juice are produced in the stomach of an adult per day.
The gastric juice of an infant contains the same components as the gastric juice of an adult: rennet, hydrochloric acid, pepsin, lipase, but their content is reduced, especially in newborns, and increases gradually. Pepsin breaks down proteins into albumins and peptones. Lipase breaks down neutral fats into fatty acids and glycerin. Rennet (the most active enzyme in infants) curdles milk (Bokonbaeva S.D. et al.).
Stomach acidity
 The main contribution to the total acidity of gastric juice is made by hydrochloric acid produced by the parietal cells of the fundic glands of the stomach, located mainly in the area of the fundus and body of the stomach. The concentration of hydrochloric acid secreted by parietal cells is the same and equal to 160 mmol/l, but the acidity of the secreted gastric juice varies due to changes in the number of functioning parietal cells and neutralization of hydrochloric acid by alkaline components of gastric juice.
The main contribution to the total acidity of gastric juice is made by hydrochloric acid produced by the parietal cells of the fundic glands of the stomach, located mainly in the area of the fundus and body of the stomach. The concentration of hydrochloric acid secreted by parietal cells is the same and equal to 160 mmol/l, but the acidity of the secreted gastric juice varies due to changes in the number of functioning parietal cells and neutralization of hydrochloric acid by alkaline components of gastric juice. Normal acidity in the lumen of the body of the stomach on an empty stomach is 1.5–2.0 pH. The acidity on the surface of the epithelial layer facing the lumen of the stomach is 1.5–2.0 pH. The acidity in the depths of the epithelial layer of the stomach is about 7.0 pH. Normal acidity in the antrum of the stomach is 1.3–7.4 pH.
Currently, the only reliable method for measuring gastric acidity is intragastric pH-metry, performed using special devices - acidogastrometers, equipped with pH probes with several pH sensors, which allows you to measure acidity simultaneously in different zones gastrointestinal tract.
Stomach acidity in conditionally healthy people(without any subjective sensations in gastroenterological terms) changes cyclically during the day. Daily fluctuations in acidity are greater in the antrum than in the body of the stomach. The main reason for such changes in acidity is the longer duration of nocturnal duodenogastric reflux (DGR) compared to daytime, which throws duodenal contents into the stomach and, thereby, reduces the acidity in the lumen of the stomach (increases pH). The table below shows the average acidity values in the antrum and body of the stomach in apparently healthy patients (Kolesnikova I.Yu., 2009):
The general acidity of gastric juice in children of the first year of life is 2.5–3 times lower than in adults. Free hydrochloric acid is determined at breastfeeding after 1–1.5 hours, and with artificial feeding – 2.5–3 hours after feeding. The acidity of gastric juice is subject to significant fluctuations depending on the nature and diet, the state of the gastrointestinal tract.
Gastric motility
In terms of motor activity, the stomach can be divided into two zones: proximal (upper) and distal (lower). There are no rhythmic contractions or peristalsis in the proximal zone. The tone of this zone depends on the fullness of the stomach. When food arrives, the tone of the muscular lining of the stomach decreases and the stomach reflexively relaxes.
 |
|
Motor activity of various parts of the stomach and duodenum (Gorban V.V. et al.)
The figure on the right shows a diagram of the fundic gland (Dubinskaya T.K.): 1 - mucus-bicarbonate layer Microflora of the stomachUntil recently, it was believed that due to the bactericidal effect of gastric juice, microflora that penetrated the stomach died within 30 minutes. However modern methods microbiological research this has been proven not to be the case. The amount of various mucosal microflora in the stomach of healthy people is 10 3 –10 4 / ml (3 lg CFU / g), including those detected in 44.4% of cases Helicobacter pylori(5.3 lg CFU/g), 55.5% - streptococci (4 lg CFU/g), 61.1% - staphylococci (3.7 lg CFU/g), 50% - lactobacilli (3. 2 lg CFU/g), in 22.2% - fungi of the genus Candida(3.5 lg CFU/g). In addition, bacteroides, corynebacteria, micrococci, etc. were sown in an amount of 2.7–3.7 lg CFU/g. It should be noted that Helicobacter pylori were determined only in association with other bacteria. The environment in the stomach turned out to be sterile in healthy people only in 10% of cases. Based on their origin, the microflora of the stomach is conventionally divided into oral-respiratory and fecal. In 2005, strains of lactobacilli that adapted (similar to Helicobacter pylori) to exist in the sharply acidic environment of the stomach: Lactobacillus gastricus, Lactobacillus antri, Lactobacillus kalixensis, Lactobacillus ultunensis. At various diseases(chronic gastritis, peptic ulcer, stomach cancer) the number and diversity of bacterial species colonizing the stomach increases significantly. In chronic gastritis, the largest amount of mucosal microflora is found in the antrum, and in peptic ulcer disease - in the periulcerous zone (in the inflammatory ridge). Moreover, the dominant position is often occupied by non- Helicobacter pylori, and streptococci, staphylococci, |